



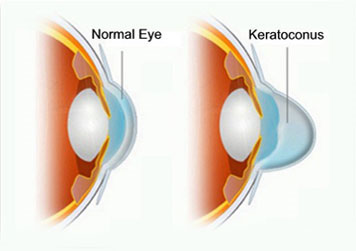
Keratoconus (KC) is an eye disease in which the central portion of the cornea begins to thin and bulge out. The resulting “cone” shape of the cornea produces a number of unique vision problems including halos, monocular double-vision, ghost images and sensitivity to light.
All the available treatment modalities for keratoconus such as Rose K contact lenses, collagen cross linking, INTACS, ICL(Implantable Collamer lens) and FEK (Femtosecond laser Enabled Keratoplasty) for scarred keratoconus eyes are available here
We have also introduced combination treatment regimens such as INTACS with collagen cross linking and topographically guided PRK( photorefractive keratectomy using Excimer laser) with collagen cross linking.
FAQ’s about keratoconus
What is Keratoconus? ( Ker-a-to-co-nus)
Keratoconus is a condition in which the normally round dome-shaped cornea (the transparent front part of the eye) progressively thins causing a cone-like bulge to develop. This results in significant visual impairment. The cornea is responsible for refracting (focussing) accurately most of the light coming into the eye. Therefore, abnormalities of the cornea severely affect the way we see the world making simple tasks, like driving, watching TV or reading a book difficult.
What is the usual age of onset of keratoconus? How fast does it progress?
The age of onset of keratoconus can vary from early teens to people in their 40′s or older. Although cases in which keratoconus is first diagnosed at an earlier age usually result in more advanced progression, it is not unusual for the disease to progress upto a certain point and then stablize. The continued thinning of the cornea usually progresses slowly for 5 to 10 years and then tends to stop. Occasionally, it is rapidly progressive.
What Causes Keratoconus?
The cause of keratoconus is still unknown despite our long experience with it. There has been no shortage of speculation or study and numerous theories have been proposed.
One scientific view is that keratoconus is developmental (i.e., genetic) in origin. This suggests that it is the consequence of an abnormality of growth, essentially a congenital defect. Another view is that KC represents a degenerative condition. Still a third view is that KC is secondary to some disease process. A less widely held hypothesis suggests that the endocrine system may be involved. This idea gained credence from the usual appearance of the disease because it is generally first detected at puberty when a lot of hormonal changes usually occur in the body.
Heredity influences in KC are suggested by studies that show that approximately 13% of patients have other family members with the disease.
Ocular allergies with associated eye rubbing has been shown to cause keratoconus.
Prabha eye clinic is equipped with the most advanced technologies available in the world for evaluating and treating all forms of Keratoconus.
Does keratoconus affect both eyes?
Yes, in approximately 90% of keratoconus cases the disease will manifest itself in both eyes. The rate of progression and the timing of the onset of the disease however is typically different for each eye.
What are the symptoms of keratoconus?
- In its earliest stages, keratoconus causes slight blurring and distortion of vision and increased sensitivity to glare and light. These symptoms usually first appear in the late teens and early twenties. Keratoconus patients can also experience light sensitivity, disturbed night vision, headaches from eye strain and reading problems. They may require frequent change of glasses.
- In the advanced stage, the patient may experience a sudden clouding of vision in one eye that clears over a period of weeks or months. This is called “acute hydrops” and is due to the sudden entry of fluid into the stretched cornea. In advanced cases, superficial scars form at the apex of the corneal bulge resulting in more vision impairment.
What are the treatment options available?
Spectacles or soft contact lenses may be used to correct the visual disturbances caused in the early stages of keratoconus. As the disorder progresses and the cornea continue to thin and change shape, rigid gas permeable contact lenses are generally prescribed to correct vision more adequately. The contact lenses must be carefully fitted, and frequent checkups and lens changes may be needed to achieve and maintain good vision.Special lenses like the Rose K lens are designed to fit properly in keratoconic eyes.
Collagen cross linking (commonly known as C3R or Accelarated cross linking- KXL) may be used in cases of progressive disease in an attempt to slow the progression.
This involves application of riboflavin eye drops and subsequent exposure of the cornea to ultra violet light of a specific frequency that is safe to the eye.
This causes an oxidative reaction and increases the cross links in the collagen fibres of the cornea , making it more rigid.
Newer surgical options in moderately advanced cases of keratoconus include INTACS and phakic ICL’s. Very advanced case of keratoconus require corneal transplant surgery.
The percentage of people that ultimately need corneal transplants for advanced disease ranges from about 16% to 22%.
Contact Lenses In Keratoconus
Keratoconus (KC) is an eye disease in which the central portion of the cornea begins to thin and bulge out. The resulting “cone” shape of the cornea produces a number of unique vision problems including halos, monocular double-vision, ghost images and sensitivity to light.
All the available treatment modalities for keratoconus such as Rose K contact lenses, collagen cross linking, INTACS, ICL(Implantable Collamer lens) and FEK (Femtosecond laser Enabled Keratoplasty) for scarred keratoconus eyes are available here
We have also introduced combination treatment regimens such as INTACS with collagen cross linking and topographically guided PRK( photorefractive keratectomy using Excimer laser) with collagen cross linking.
Why is my vision sometimes more than “double”? I only have 2 eyes so where do the other images come from?
Multiple images can be caused by many different causes. They can be because of a disparity between the two eyes or from multiple refractive zones within the optical zone of just one eye. If you see double and it disappears when you close either eye it is most likely a binocular problem caused by the two eyes not working together. The causes of this are many and some are potentially serious. Multiple images seen only in one eye i.e even when the other eye is closed occur more frequently in diseases affecting the cornea, lens or iris of the eye. In keratoconus, surface thinning can create multiple optical zones that individually focus the same image to different areas of the retina, thus creating the additional perceived images. Contact lenses will usually eliminate much of this distortion.
Will I go completely blind?
No, very few if any persons suffer from total blindness from keratoconus alone. But in severe cases, one’s vision can be significantly impaired and normal everyday activities may be difficult. However with the currently available treatment options most patients retain useful vision enabling them to lead normal productive lives.
What is astigmatism? Are keratoconus and astigmatism same?
Astigmatism is a common condition where the curvature of one or more of the optical surfaces of the eye (the cornea and lens surfaces) are more “round” in one direction than the other. In “regular” astigmatism the maximum and minimum powers are aligned at 90 degrees to each other while in “irregular” astigmatism they do not align. An egg is a good example of a surface with “regular astigmatism”. Keratoconus is a degenerative condition where the cornea thins in certain areas. This can lead to astigmatism – often regular at first but becoming increasingly irregular as the disease progresses.
Astigmatism is expressed in terms of diopters. Astigmatism between 0.25 and 2.00 diopters is not unusual amongst the normal population. Between 2.25 and 3.75 diopters is less common but still seen. Much above that in a “normal” person is unusual. Keratoconus and post-transplant patients can have 10 D or even more of astigmatism.